
Testing, Labs, and Why MCAS Is So Difficult to Confirm
For many people experiencing Mast Cell Activation Syndrome (MCAS), the path to diagnosis can be long and confusing. Patients often move from specialist to specialist, undergo repeated testing, and still feel that their symptoms remain unexplained. This experience is not unusual. MCAS is widely considered one of the most challenging chronic conditions to identify because it does not follow the traditional rules of diagnosis.
Unlike conditions that can be confirmed with a single laboratory value or imaging test, mast cell activation is dynamic. Symptoms may come and go, laboratory markers fluctuate, and many patients appear “normal” on routine testing. Understanding how MCAS is evaluated, and why diagnosis can be complex, can help patients and practitioners approach the process with realistic expectations and a clearer sense of direction.
Why MCAS Does Not Have a Single Definitive Test
Modern medicine often relies on clear diagnostic markers. A condition such as diabetes can be confirmed with blood glucose measurements. Many infections can be identified through specific laboratory tests. MCAS, however, does not fit neatly into this framework.
Mast cells are immune cells distributed throughout the body, particularly in the skin, digestive tract, respiratory system, and nervous system. Their role is to detect potential threats and release chemical mediators that help the body respond. In MCAS, these cells become overly reactive and release inflammatory chemicals inappropriately or excessively.
The difficulty arises because mast cells release dozens of different mediators, and these mediators are not consistently elevated. Levels may spike only during symptom flares and return to normal afterward. If testing is performed during a quiet period, laboratory results may not reflect the underlying problem.
This fluctuating nature of mast cell activity explains why many patients are told their test results are normal despite ongoing symptoms.
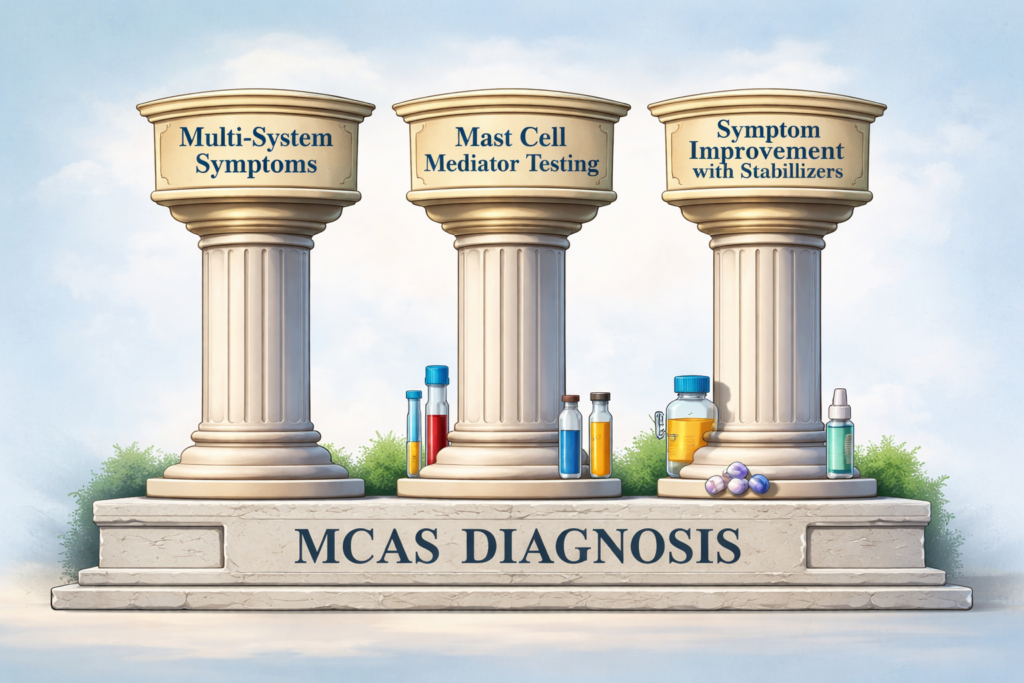
Understanding the Three Pillars of MCAS Diagnosis
Because no single test can confirm MCAS, many clinicians rely on a framework that combines symptom patterns, laboratory evidence, and treatment response. This approach helps differentiate MCAS from allergies, autoimmune disease, and other chronic conditions.
First Pillar of MCAS Diagnosis: Multi-System Symptoms
MCAS typically affects multiple body systems at once. Patients may experience digestive issues, skin reactions, neurological symptoms, cardiovascular changes, or respiratory discomfort. The wide range of symptoms often leads to fragmented care, with each system evaluated separately.
Recognizing the pattern of multi-system involvement is a key step toward identifying mast cell activation.
Second Pillar of MCAS Diagnosis: Evidence of Mast Cell Mediator Release
Laboratory testing focuses on identifying chemical mediators released by mast cells. While these markers can provide valuable clues, they are not always elevated and must be interpreted carefully.
Third Pillar of MCAS Diagnosis: Symptom Improvement With Mast Cell Stabilization
In some cases, symptom improvement after mast-cell–targeted support becomes an important part of the diagnostic picture. Because laboratory confirmation of MCAS can be inconsistent, many experienced clinicians also observe how a patient responds to interventions that reduce histamine burden and calm mast cell activity.
When patients experience meaningful improvement with a low-histamine diet and appropriate use of H1 and H2 antihistamines, it can provide supportive clinical evidence that mast cell mediators and histamine intolerance may be contributing to their symptoms. While this response alone does not confirm MCAS, it often helps guide clinical suspicion and next steps.
In practice, physicians may recommend a monitored trial of H1 blockers such as hydroxyzine, doxepin, loratadine, fexofenadine, diphenhydramine, ketotifen, or cetirizine, often paired with an H2 blocker such as famotidine (most commonly used due to its lower risk of drug interactions), cimetidine, or ranitidine where available. Some patients may also benefit from mast cell stabilizers such as cromolyn or ketotifen, and in select cases leukotriene inhibitors like montelukast or zafirlukast may be considered.
For best effect, H1 and H2 blockers are often dosed consistently (commonly every 12 hours), and clinical response may take time to fully emerge. In certain cases and under physician supervision, dosing may be carefully titrated above standard over-the-counter levels based on patient response and tolerance.
Dietary intervention can also provide useful clinical insight. Many clinicians will evaluate how a patient responds to a low-histamine dietary approach, which reduces common sources of exogenous histamine. This typically involves limiting foods such as alcohol, smoked and cured meats, canned fish, fermented and pickled foods, aged cheeses, chocolate, citrus, tomatoes, vinegar-containing foods, and leftovers that have been stored for extended periods.
It is important to recognize that a low-histamine diet primarily reduces incoming histamine load and does not directly correct mast cell overactivation. However, when patients notice clear symptom improvement with dietary histamine reduction in combination with H1 and H2 blockade, it can be a meaningful clinical clue that histamine and mast cell activity are playing a role in their symptom pattern.
Because responses vary widely, these interventions should always be individualized and guided by a knowledgeable clinician.
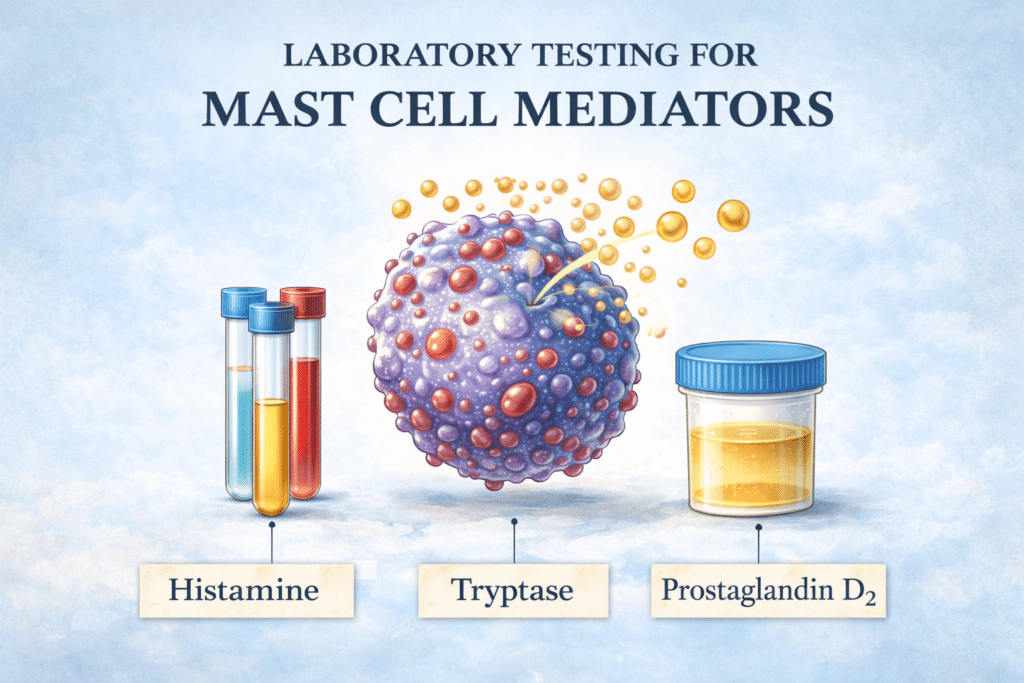
Laboratory Testing for Mast Cell Activation
Laboratory evaluation focuses on substances released during mast cell activation. These mediators can be measured in blood or urine, although each test has limitations.
Serum Tryptase
Tryptase is one of the most well-known mast cell markers and is commonly used in evaluating mast cell disorders. Elevated tryptase levels are strongly associated with mastocytosis, a rare condition involving abnormal mast cell accumulation.
However, many individuals with MCAS have normal tryptase levels, particularly when testing occurs outside of severe reactions. This makes tryptase helpful but not definitive.
Histamine Testing
Histamine is one of the primary mediators released by mast cells and is responsible for many allergic-type symptoms. Measuring histamine levels can provide useful information, but the process is challenging. Histamine breaks down quickly in the bloodstream, and improper handling of samples can affect results.
Because of this, histamine testing must be carefully timed and interpreted in context.
Prostaglandins and Leukotrienes
Prostaglandin D2 and leukotrienes are inflammatory compounds that can indicate mast cell activation. These markers may be measured through blood or urine testing and are often evaluated alongside histamine.
Although these markers can support the diagnosis, they are not specific to MCAS and may be influenced by other inflammatory conditions.
24-Hour Urine Testing
Urine testing attempts to capture mediator release over a longer period of time. Measuring metabolites such as N-methylhistamine or prostaglandin breakdown products can help identify patterns that single blood tests might miss.
Even with this approach, results may still fluctuate depending on symptom activity.
Discuss Targeted Laboratory Testing With Your Physician
Confirming MCAS through laboratory testing can be challenging because mediator levels often rise and fall with symptom activity. As a result, testing performed during relatively calm periods may miss active mast cell mediator release. For some patients, repeat testing during symptomatic flares is necessary to capture meaningful abnormalities.
Another important limitation is specimen handling. Many mast cell mediators are extremely fragile and require immediate chilling and rapid processing. If samples are not handled correctly, results may appear within normal range even when the clinical picture strongly suggests mast cell activation.
It is also important to recognize that MCAS does not consistently produce abnormal laboratory findings. In real-world clinical practice, clearly positive mediator results are identified in only a portion of suspected cases. For this reason, laboratory data must always be interpreted alongside the patient’s full clinical presentation.
If you and your physician are pursuing evaluation for possible MCAS, the following studies are commonly used. The first group represents the core mediators most frequently relied upon in diagnostic workups.
Core Mast Cell Mediator Testing
Histamine — plasma (Quest 36586)
Specimen must remain chilled.
N-Methylhistamine — 24-hour urine
Specimen must remain chilled.
Prostaglandin D2 (PGD2) — plasma
Requires chilled handling. NSAIDs and aspirin should typically be avoided for approximately five days beforehand under physician guidance.
Prostaglandin D2 (PGD2) — 24-hour urine
Chilled collection required; avoid NSAIDs and aspirin prior to testing.
Chromogranin A (Quest 16379)
Proton pump inhibitors and H2 blockers can falsely elevate results and are often held for about five days beforehand with medical supervision.
Additional Mast Cell–Associated Markers
Additional supportive testing may include:
- Prostaglandin 11-beta F2 alpha (PGF2α) — 24-hour urine
- Serum tryptase (Quest 34484)
- Leukotriene E4 — 24-hour urine
- Plasma heparin Anti-Xa
- Coagulation studies (Thrombin, PT, PTT, INR)
- Anti-IgE receptor antibody
- Neuron-specific enolase (Quest 34476)
- Plasma pheochromocytoma evaluation
- Porphyria screening
- Factor VIII assessment
- Plasma free norepinephrine (Quest 37562)
- Urinary metanephrines
- Immunoglobulins (IgG, IgM, IgE, IgA)
- Gastrin
- Ferritin
- CBC with differential (including eosinophils and basophils)
- Antiphospholipid antibodies
When clinically indicated, a bone marrow biopsy evaluating markers such as CD117/CD25 or CD117/CD2 may be considered to rule out systemic mastocytosis.
Genetic and Functional Considerations
In selected patients, clinicians may also explore factors that influence histamine metabolism and detoxification capacity. These may include:
- MTHFR gene variants
- MAT gene variants
- DAO gene variants
- HNMT gene variants
- Glutathione status
- Zonulin and DAO enzyme testing
The liver contributes to histamine clearance through the HNMT pathway. When glutathione stores are depleted, the body may be less able to neutralize inflammatory mediators released by mast cells, potentially perpetuating oxidative stress and inflammatory signaling.
Important note: Because many mast cell mediators degrade rapidly, proper collection, chilling, and timely processing of specimens are essential for reliable results.
Why MCAS Lab Results Are Often Normal
One of the most frustrating aspects of MCAS is the disconnect between symptoms and laboratory findings. Many patients undergo extensive testing only to be told that results are normal.
This does not necessarily mean mast cells are functioning normally. Instead, it reflects the episodic nature of mast cell activation. Testing during a period of relative stability may not capture the biochemical changes occurring during flares.
This reality underscores the importance of evaluating the whole clinical picture rather than relying on a single laboratory value.
The Importance of Clinical Evaluation
Because of testing limitations, clinical history plays a central role in MCAS diagnosis. Practitioners often look for patterns that suggest immune system dysregulation and abnormal reactivity.
Common patterns include:
- Sensitivity to foods or medications
- Reactions to temperature or stress
- Long history of unexplained symptoms
- Fluctuating symptom severity
These patterns help clinicians identify mast cell involvement even when laboratory evidence is limited.
Conditions That May Overlap With MCAS
MCAS can resemble or coexist with several other conditions, which contributes to diagnostic complexity. Patients may initially be evaluated for allergies, digestive disorders, anxiety, or autoimmune disease before mast cell activation is considered.
Understanding this overlap helps explain why diagnosis often takes time and why a comprehensive approach is necessary.
Why Diagnosis Matters
Identifying mast cell activation can provide an important framework for understanding chronic symptoms. Recognizing the role of mast cells may help patients better understand triggers, improve treatment tolerance, and reduce severe reactions.
Although diagnosis can be complex, gaining clarity about mast cell involvement often represents a turning point in understanding chronic illness.
Summary
MCAS diagnosis requires a combination of symptom history, laboratory testing, and clinical evaluation. No single test can confirm or rule out the condition, and results must be interpreted within the broader clinical context.
Recognizing the limitations of testing can help patients approach the diagnostic process with greater clarity and realistic expectations.


